

What is acute angle closure glaucoma? When the fluid pressure inside of your eye rapidly increases, it can lead to acute angle-closure glaucoma, a serious eye disorder. A red eye, sudden, intense eye pain, and decreased or blurred vision are the typical symptoms. You may feel sick to your stomach. To alleviate symptoms and stop irreversible eyesight loss, treatment must be started very away.
Angle-closure is the iris’s attachment to the trabecular meshwork, which raises the intraocular pressure (IOP). Acute angle closure (AAC) symptoms, which include blurry vision, red eyes, pain, headaches, nausea, and vomiting, appear suddenly and dramatically. Acute angle-closure glaucoma can soon develop as a result of the abrupt and significant IOP increase damaging the optic nerve (AACG).
A delay in treatment for AAC, a true ophthalmic emergency, could cause blindness. The best treatment is to prevent it from occurring in susceptible individuals, while prompt treatment can occasionally reduce the degree of vision loss.
What causes Acute Angle Closure Glaucoma?
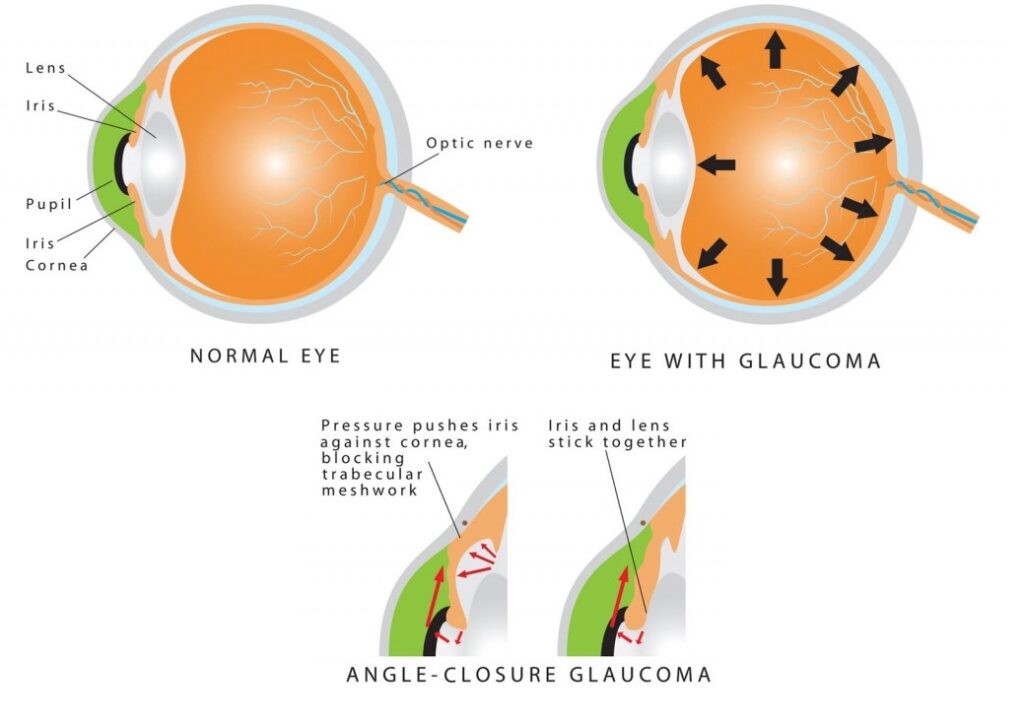
Pupillary block is a mechanism that causes AAC. The ciliary body normally produces aqueous humor, which then passes through the pupil and into the anterior chamber before draining into the trabecular meshwork to leave the eye. The iris and the lens can come into contact with one another in those who are at risk for angle closure because the distance between them is at its shortest when the pupil is mid-dilated. When this happens, the iris is forced forward because the aqueous humor cannot pass through the pupil and into the anterior chamber (pupillary block). The aqueous humor cannot exit the eye (angle closure) when the iris is compressed against the trabecular meshwork, raising IOP.
IOP is typically 10–21 mm Hg. IOP in AAC frequently exceeds 40 mm Hg. IOP damage that is rapid and severe can result in irreparable optic nerve damage very fast (acute angle-closure glaucoma).
In addition to the pupillary block, other factors such as a plateau iris, the use of specific drugs, increased iris thickness, increased iris volume with dilatation, hyperopia, and increased lens thickness in cases of phacomorphic angle closure can also cause primary angle closure.
If the episode of pupillary block recovers spontaneously after a short period of time (a few hours), typically after sleeping supine, intermittent angle-closure glaucoma develops.
If the angle gradually narrows, scarring between the periphery of the iris and the trabecular meshwork occurs; the IOP steadily rises as this occurs.
Any person with narrow angles who experiences pupillary dilatation (mydriasis) may cause the iris to enter the angle and develop acute angle-closure glaucoma. This change is especially concerning when systemic medications that have the ability to enlarge the pupils are administered (eg, scopolamine for motion sickness, alpha-adrenergic agonists commonly used to treat urinary incontinence, anticholinergics). , as well as when topical agents are used to enlarging the pupils of the eye for therapy or examination (homatropine, tropicamide, phenylephrine, etc).
Medications used frequently that could cause acute glaucoma
- Eye drops that enlarge the pupil may be used during eye exams.
- Tricyclic or selective serotonin reuptake inhibitor (SSRI) antidepressants.
- Some of the medications are used to treat nausea and vomiting, as well as schizophrenia, a mental health illness. (Chlorpromazine is a member of the class of drugs known as phenothiazines.)
- Ipratropium is used for asthma.
- Topiramate is prescribed for migraines and seizures.
- Some medications, including ranitidine, cimetidine, and chlorphenamine, are used to treat stomach ulcers or allergies.
- Drugs used when under a general anesthetic.
- When used for extended periods of time, steroid medications (such as those used to treat asthma and emphysema) can occasionally produce high eye pressure, but they typically do not result in acute glaucoma.
Angle-closure secondary glaucomas
A concomitant disease, such as proliferative diabetic retinopathy (PDR), ischemic central vein occlusion, uveitis, or epithelial down-growth, is the cause of the mechanical obstruction of the angle. The iris may be pulled into the angle by the contraction of a neovascular membrane (such as in PDR) or by inflammatory scarring.
Risk Factors and Prevalence
Fortunately, acute glaucoma is a rare illness that only affects one in 1,000 individuals. Persons above the age of 40 are more at risk, yet it typically occurs in people between the ages of 60 and 70. Women and people with hyperopia (far-sighted) are more likely to experience it. Additionally, Southeast Asians and Inuits are more likely to have it.
You are more likely to get acute glaucoma if one of your close relatives (mother, father, sister, or brother) has had it. This is because you might have inherited an eye shape that increases your risk of developing acute glaucoma. When and how often you should get eye exams should be discussed with an eye doctor if you have it in the family history.
Angle-Closure Glaucoma Symptoms and Signs
Glaucoma with acute angle-closure
Severe ocular pain and redness, blurred vision, colored halo rings surrounding lights, headaches, nausea, and vomiting are all common in patients. Systemic problems may be so severe that patients receive a false diagnosis of a neurological or digestive issue. Anterior chamber inflammation, a cloudy cornea, a fixed mid-dilated pupil, and conjunctival hyperemia are common findings during examination. The patient’s vision is impaired. IOP (intraocular pressure) is typically measured between 40 and 80 mm Hg. The corneal edema makes it challenging to see the optic nerve, and discomfort prevents visual field testing. The diagnosis for basic mechanisms of angle closure (such as pupillary block and plateau iris) can be determined by examining the contralateral eye that is not affected.
Chronic angle-closure glaucoma
Comparable to open-angle glaucoma, this kind of glaucoma has similar symptoms. Some people have headaches, ocular redness, discomfort, or blurred vision, which subside after sleep (perhaps because of sleep-induced miosis (pupil constriction) and shifting rearward of the lens by gravity). The angle is small on gonioscopy, and peripheral anterior synechiae, commonly known as PAS (adhesions between the peripheral iris and angle structure causing occlusion of the trabecular meshwork and/or ciliary body face), may be visible. IOP in the afflicted eye is often greater but could be normal.
Prognosis
With early discovery and treatment, the prognosis is good. Treating vulnerable people before AAC is the most effective strategy to stop vision loss.
Diagnosis
Patients who have suspected AAC should get a thorough ocular examination. The focus of this test should be on the patient’s vision, pupil, gonioscopy, tonometry, slit-lamp examination, and evaluation of the optic nerve:
The diagnosis of AAC is made based on a gonioscopic vision of a narrow occludable angle in the contralateral unaffected eye and an occluded anterior chamber angle in the affected eye.
Tonometry shows an increased IOP that may range from 40 to 80 mm Hg in the affected eye.
A shallow anterior chamber, conjunctival injection, a fixed or sluggish and mid-dilated pupil, corneal epithelial edema and bullae, cells, and flare may all be seen during a slit-lamp examination. The eye may be weeping and closed, and the patient may be quite sensitive to light.
If there has been a history of recurrent or chronic episodes, ophthalmoscopy may show a swollen optic disc during an acute attack or cupping of the nerve. In AAC, unilateral involvement and symptoms that intensify frequently occur.
The following could be seen if angle closure episodes have previously taken place:
- Adhesions between the iris and trabecular meshwork as well as between the lens and posterior are known as synechiae.
- Vesicles on The front of the lens called Glaucoma flecks
- Iris atrophy
Treatment for acute angle-closure glaucoma
Treatment for the acute occurrence
Acute glaucoma requires prompt medical attention. You need to see an eye doctor as soon as you can. The beginning of treatment is possible even if it takes some time to reach the ophthalmologist.
You shouldn’t attempt to use a patch or a blindfold to cover the injured eye. Your pupil will enlarge more if you do this, which could make the condition worse. Avoid lying down in a pitch-black environment because doing so tends to make your eye pressure worse. The situation will worsen in a dark environment since the pupil will expand even more.
Medication to reduce the pressure inside of your eye is the first course of treatment. Eye drops and medications come in a variety of combinations that can be used in various ways. Treatments could consist of:
- Beta-blocker eye drops, such as timolol to lower the pressure in the eye, and also a steroid to lessen inflammation such as the administration of acetazolamide through injection.
- Pilocarpine eye drops can help to shift the iris away from the trabecular meshwork by making your pupil smaller (constrict). This aids in clearing the way for the flow of aqueous humor fluid.
- Steroid eye drops and other varieties are also employed.
- Other diuretics include mannitol, which is injected into a vein (intravenously).
- If necessary, you may also receive painkillers and anti-sickness medication.
Additional therapy
Additional therapy is required after your eye’s pressure has decreased to prevent acute glaucoma from returning. Making a tiny hole in your iris requires laser therapy or surgery. The opening permits fluid to freely circulate around your iris and can prevent future iris forward bulges that would impede the trabecular meshwork.
Peripheral iridotomy is the term for laser therapy. This is the standard course of action. Usually, a laser is used to create two tiny holes in your iris. Other people will likely hardly even notice the holes. In an outpatient facility, laser therapy is performed while under local anesthetic.
Another possibility is a procedure called a surgical iridectomy. It creates a tiny, triangular hole in your iris. Afterward, the hole appears as a tiny, black triangle at the edge of your iris.
Typically, laser or surgical therapy is suggested for the opposite eye, frequently concurrently. This will avoid what would otherwise be a very likely occurrence of acute glaucoma in the opposite eye. Sometimes using eye drops over a longer period of time is necessary to maintain control of your eye pressure.
Long-Term Treatment
After the initial acute angle closure (AAC), the patient needs to be closely watched to make sure of the following:
- The IOP returns to normal, and AAC stops happening.
- Once the anterior chamber is sufficiently visible, do laser iridotomy.
- Verify the laser treatment’s efficacy and determine whether additional treatment, like iridoplasty, is necessary.
- Treatment should continue until the patient’s pupil and vision return to normal and the inflammation has subsided. Taper the medicine dosage gradually.
- Examine the opposite eye and administer laser therapy as necessary.
Conclusion
As with most medical conditions, prevention is so important. Having regular eye exams to determine if you are at risk for acute angle glaucoma or any other type of eye disease will greatly reduce your chances of losing your vision to this condition. If you are aware of the possibility of the condition happening and the signs and symptoms of that condition, you can take immediate action to prevent sight loss.
FAQ’s
Acute angle-closure glaucoma: how serious is it?
It’s a medical emergency. The excessive pressure could permanently harm your vision if it is not lowered within a few hours. A hospital emergency department or your eye doctor should be visited immediately if you notice any of these signs.
How fast does angle-closure glaucoma develop?
It can rise (the pressure) in just a few hours. It occurs when the fluid in your eye is unable to drain properly. It is less frequent than other forms of glaucoma, which gradually increase pressure over time.
Could closed-angle glaucoma cause blindness?
As a result of the increased pressure and subsequent nerve damage, your vision gradually deteriorates. Open-angle glaucoma and acute angle-closure glaucoma are the two most prevalent kinds of glaucoma. Every type of glaucoma reduces vision and, if left untreated, can result in blindness.








