Cotton-wool spots are localized accumulations of axoplasmic debris in the retinal nerve-fiber layer caused by interrupted axonal transport, most often seen among patients suffering from diabetes and high blood pressure, and an early warning sign for progression towards proliferative diabetic retinopathy if left untreated properly.
These white spots are caused by small blood vessel occlusions that result in swelling of the retina (macular edema). They may appear as non-symptomatic areas or may accompany other symptoms, such as hemorrhages.
Causes
Cotton wool spots (CWS) are white or grayish lesions on the retina, the layer of light-sensing cells lining the back of the eye, that result from inadequate blood flow to retinal nerve fibers, leading to their swelling and degeneration resulting in fluffy white spots on an eye exam. CWS are not diseases in themselves nor pose an imminent threat to vision; rather they offer clues to an underlying systemic medical condition which could have both systemic and ocular consequences; for this reason CWS should not be ignored and work-up should usually be undertaken immediately.
CWS can be an indicator of an underlying medical condition, most frequently diabetes and hypertension, since both are known to lead to changes such as CWS in patients. Diabetics in particular should watch for CWS as this often marks microvascular damage associated with their disease – left untreated it may result in proliferative diabetic retinopathy leading to permanent vision loss. CWS have also been found as an early indicator for HIV related ocular and systemic complications in their bodies.
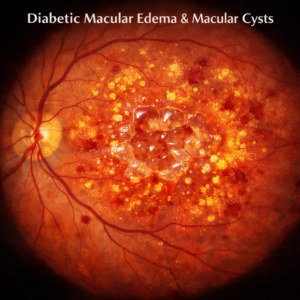
Cotton-wool spots are deposits of fluids and lipids leaking from damaged blood vessels in the retina. When these leakage fluids collect in areas near the macula (where fine detail and reading take place), this condition is known as macular edema and its severity directly correlated to length and degree of diabetes as well as compliance with medical recommendations, particularly blood pressure control recommendations. Cotton-wool spots may also serve as early warning signals of proliferative diabetic retinopathy – an advanced form of diabetic retinopathy.
Cotton-wool spots may be caused by arterial occlusive disease such as aortic dissection), sclerosing cholangitis, vasculopathies like giant cell arteritis, polymyalgia rheumatica or collagen diseases like Lupus Erythematosus; to accurately assess these diseases a thorough history and ocular exam must be performed with specific questioning for assessment; tests may include complete blood count analysis (CBC), HbA1c levels (HbA1c), comprehensive metabolic panel evaluation and evaluation for inflammation markers like ESR/Creactive protein evaluation.
Diagnosis
Cotton wool spots can be diagnosed through patient history and physical exam. Cotton wool spots serve as indicators of systemic illness; their formation results from blockage of axoplasmic flow through retinal blood vessels leading to interruption of retinal nerve fiber layer function and an ischemic interruption. Cotton wool spots often accompany other signs of vascular disease such as hemorrhages (see image) or arcuate defects in visual field.
Cotton-wool spots are a telltale sign of proliferative diabetic retinopathy, which can result in blindness. Cotton-wool spots are also often seen among HIV retinopathy cases and can serve as an early indicator of infection severity.
A 50-year-old man presented to an ophthalmologist with newly emerging floaters in both eyes. A fundus examination revealed scattered, large cotton wool spots centrally within his retina accompanied by diffuse whitening in this area; no other symptoms suggestive of diabetes or hypertension were noted in either eye.
Ophthalmologist was alarmed at this constellation of findings, particularly given the patient’s history of polymyalgia rheumatica and positive Westergren erythrocyte sediment rate. After performing temporal artery biopsy to confirm giant cell arteritis diagnosis and subsequent cotton-wool spot removal following treatment with corticosteroids.
Cotton-wool spots tend to be symptom-free in patients, especially if they occur away from the center of the macula. However, their appearance should prompt a thorough ophthalmological exam as well as systemic work-up. This should include taking vitals, ordering a complete blood count with differential and peripheral blood smear, checking inflammatory markers like ESR and CRP, performing cardiovascular assessment with electrocardiogram, echocardiogram and carotid ultrasound as well as protein electrophoresis and pancreatic enzyme analysis; when applicable intravenous fluorescein angiography may help confirm and identify additional aspects of retinal vascular disease such as microaneurysms or vasculitis.
Treatment
Cotton wool spots do not necessarily warrant treatment in and of themselves; rather they serve as a sign that systemic disease exists and should prompt additional testing – these tests might include complete blood count with differential, comprehensive metabolic panel or peripheral blood smear test; additionally if the individual has had blood dyscrasias in the past then plasma protein electrophoresis testing might also be undertaken.
Cotton-wool spots are localized accumulations of axoplasmic debris within bundles of unmyelinated retinal nerve cell axons, typically less than one quarter the size of an optic disc, found within retinal nerve fiber layers in peripheral areas. It is thought that cotton-wool spots arise due to small vessel obstruction leading to interruptions of axonal transport similar to brain ischemic events resulting in swelling axons that ultimately form puffy white spots on retinal nerve layers.
Cotton-wool spots may not interfere with vision directly, but they should prompt a full medical evaluation for further assessment. Diabetes and hypertension patients are at higher risk for cotton-wool spots as well as more serious diabetic retinopathy including proliferative retinopathy; managing either condition effectively should alleviate symptoms while further more serious forms of retinopathy will likely be prevented from emerging.
Cotton-wool spots may also result from chronic myelogenous leukemia, sarcoidosis and vasculitis – particularly venous vasculopathy – as well as various other conditions. These patients frequently present with associated vitreous hemorrhage, microaneurysms and other retinal vascular changes which must be diagnosed and treated as soon as possible. These patients require an intensive evaluation, including testing for glycated hemoglobin, metabolic panel testing, EKG and echocardiogram screening, CRP and ESR levels as well as other inflammation markers like CRP/ESR levels. As these conditions can develop into more serious ocular and systemic complications, such as progression to severe retinopathy, vision loss, stroke or cardiovascular disease without treatment, further assessments such as carotid ultrasound or blood pressure monitoring may also be required for further treatment. Left untreated they can lead to even more serious consequences including progression into severe retinopathy, vision loss, stroke or cardiovascular disease – potentially even leading to death.
Prevention
Cotton wool spots are not diseases in themselves, but can serve as indicators for systemic health problems that need treatment. Cotton wool spots may indicate conditions affecting blood vessels such as diabetes or hypertension that require treatment; more severe forms of diabetic retinopathy – proliferative diabetic retinopathy in particular – or HIV infections that require medical intervention to manage. Cotton wool spots may also serve as indicators of HIV infection with potential consequences including HIV-associated ocular disease like Cytomegalovirus Retinitis.
Cotton-wool spots are small, fluffy white or grayish lesions found on the retina — the layer of cells at the back of the eye responsible for turning light into neural signals that travel to the brain. Cotton-wool spots usually represent localized ischemia or insufficient blood supply to retinal nerve fibers which causes swelling and loss of structure of these fibers resulting in fuzzy white patches on retina during an eye examination.
Exudates, which consist of more viscous fluid made up of proteinaceous material and can be seen in conditions such as diabetic retinopathy, are different than CWS as they indicate poor blood circulation within the retina and both can result in visual impairment if left untreated. CWS management includes treating its source and regularly receiving eye exams to prevent recurrence; failing this, CWS could recur, leading to blurry vision, scotomas or even transient vision loss known as amaurosis fugax.