Long-term use of blood pressure medications can damage blood vessels in the eye – an effect known as hypertensive retinopathy.
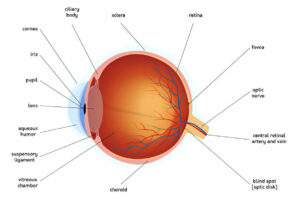
The retina is a light-sensitive layer located at the back of your eye, and chronic hypertension can lead to mini-vascular accidents in its blood vessels, known as hypertensive retinopathy.
Treatment
The retina, the light-sensitive tissue at the back of your eye responsible for transmitting visual signals to the brain, can be damaged by chronic, uncontrolled high blood pressure. This condition is known as hypertensive retinopathy; high blood pressure exerts excessive force on eye blood vessels which exert excessive strain and cause them to narrow or even rupture, eventually leading to hypertensive retinopathy and leading to retinal sclerosis which in turn results in hypertensive retinopathy.
Hypertension is a potentially life-threatening condition. Left untreated, it can lead to heart attack, stroke, kidney failure and damage to other organs in the body. Treatment for systemic hypertension aims at long-term reduction of blood pressure; lifestyle modifications often suffice as treatment in terms of keeping hypertension at manageable levels while simultaneously preventing further development that could threaten vision or other organs in the body.
Research demonstrates that blood vessel changes caused by hypertension are an excellent predictor of cardiovascular disease risk factors overall. For instance, the Beaver Dam Eye Study revealed that people with elevated blood pressure were 50-70% more likely to have retinal hemorrhages and microaneurysms, as well as 30-40% more likely to exhibit focal arteriolar narrowing or arteriovenous nicking than those without elevated blood pressure levels.
Hypertensive retinopathy is graded according to its severity when diagnosed. Grades 1-3 exhibit mild blood vessel changes with some leaking or swelling, while grade 4 features optic disk and macula swelling with cotton wool spots or hard exudates; left untreated, hypertensive retinopathy can lead to permanent vision loss.
Doctors can lower vision loss risk by treating hypertensive retinopathy with lower blood pressure. This approach is the best way to stop further complications from occurring.
At first, it is necessary to determine whether systemic hypertension exists. An ophthalmologist or other health care provider takes a detailed history of blood pressure levels and medication use before conducting a full ocular examination involving examination of retina (the transparent layer at the back of eye) for signs of hypertension such as large arteries or veins in retina; an ophthalmoscope measures size of blood vessels within retina.
Diagnosis
Hypertensive Retinopathy may go undetected for some time; however, uncontrolled high blood pressure can damage small blood vessels in the retina over time and lead to vision loss in patches of one eye. Furthermore, this signifies that cardiovascular issues like heart disease or stroke could arise as a result.
Hypertensive retinopathy‘s severity is determined by the extent of damage to retinal blood vessels observed with an ophthalmoscope. With mild changes, vision loss risk remains low; however, as hypertension continues and blood pressure rises further, so too do its consequences – when severe changes cause optic disk and macula swelling known as “papilledema” which could eventually lead to permanent blindness if left untreated.
Diagnosing hypertensive retinopathy involves conducting a complete eye exam that includes both a visual field test and examination of retinal blood vessels using an ophthalmoscope. The degree of retinopathy directly corresponds with damage done to other parts of the body such as kidneys or the heart.
Research has demonstrated the correlation between severity of hypertensive retinopathy and risk for cardiovascular diseases and its severity in an individual. Mild hypertensive retinopathy signs (including generalized or focal retinal arteriolar narrowing, arteriovenous nicking and microaneurysms) are weakly associated with systemic vascular disease in older populations while moderate signs have strong links with subclinical and clinical cardiovascular conditions like stroke, coronary heart disease and congestive heart failure despite traditional risk factors
Treatment of hypertensive retinopathy involves controlling blood pressure. Doctors may prescribe beta blockers, diuretics and calcium channel blockers to lower it; angiotensin receptor antagonists and angiotensin converting enzyme inhibitors may be prescribed in more serious cases of hypertensive retinopathy. Patients should abide by their medical regimen and stay in touch with their primary care physician regularly for monitoring purposes.
Medications
Hypertension, or high blood pressure, places an excessive force on the eye’s blood vessels. This results in hypertensive retinopathy – damage to retinal blood vessels which allows fluid leakage into surrounding tissue which results in blurred vision or even blindness if left untreated. Hypertensive retinopathy also poses risks of kidney disease and heart failure as well.
Diet, exercise and medication are among the best means of controlling hypertensive retinopathy; particularly important among younger patients whose retinal blood vessels have not become rigid. Doing this reduces their chances of compensatory changes such as arteriolar narrowing and AV nicking.
Although diabetic retinopathy can be devastating, diabetic-retinopathy-like retinopathy should not be overlooked either. Patients must keep their blood pressure under control and regularly visit an ophthalmologist so that early signs of damage to blood vessels can be identified and treatments offered to ensure further deterioration to vision or other aspects of health.
Not many hypertensive patients realize the damage their chronic hypertension can do to their eyes, leading them to forego getting eye examinations or treatments – leading to further progression of symptoms over time. Treatment typically entails taking targeted blood pressure-reducing drugs like angiotensin converting enzyme inhibitors and calcium channel blockers.
Studies have revealed that hypertensive retinopathy severity is strongly related to systemic cardiovascular diseases. Mild retinopathy, such as generalized and focal arteriolar narrowing and arteriovenous nicking, is only weakly associated with cardiovascular diseases. Moderate hypertensive retinopathy symptoms like retinal hemorrhages, cotton wool spots and microaneurysms have long been linked with subclinical and clinical cardiovascular conditions. Therefore, it is vital that all patients adhere to international blood pressure control guidelines and receive frequent eye examinations in order to facilitate early diagnosis and referral for cardiovascular risk assessment and management.
Surgery
High blood pressure (hypertension) damages the retina (the light-sensitive layer at the back of the eye). Over time, hypertension causes its vessels to thicken and no longer transport blood efficiently into various areas of the retina, leaving some vulnerable areas vulnerable to bleeding and leakage resulting in blot-like, dot-like or flame-shaped hemorrhages and hard exudates (cotton wool spots). Furthermore, central retinal vein occlusion or other smaller branch vein obstruction may occur causing macular edema.
Hypertensive retinopathy may range in severity from mild to severe; medication to reduce blood pressure is usually used as the main form of treatment, in partnership with your primary care physician and ophthalmologist, who will work together for proper follow-up of patients who require therapy.
The Beaver Dam Eye Study revealed that those who did not control their blood pressure with medication were 50 to 70% more likely to develop retinopathy than those who did, with lower blood pressures associated with reduced retinal vessel damage and visual loss. The severity of retinopathy symptoms corresponds directly with blood pressure level; those without medically managed blood pressure were much more likely to experience its symptoms and experience them more severely than those who managed theirs via medication.
Untreated leakage of blood vessels may lead to macula swelling (macular edema), potentially leading to severe vision loss in the center of your field and necessitating regular dilated retinal exams for diagnosis and management. Ophthalmologists use ultrasound to monitor fluid leakage and its progression of eye disease. If fluid is leaking out, treatment options include laser surgery or intravitreal injection of vascular endothelial growth factor (VEGF) drugs to stop further visual degradation and stop further leakage. At times, retinal veins may become clogged with clots or plaque, which is treatable with VEGF injections or laser treatment. If these treatments fail to improve vision, surgery may be performed to extract clots from within the retina – this invasive procedure has a better chance of improving vision than its alternatives.