Cholesterol often takes the blame for increasing heart disease risks, but high levels of this lipid can also have devastating effects on eyesight. One way in which cholesterol manifests itself in eyesight is through xanthelasma deposits which appear as yellow fatty deposits on skin around eyes.
Xanthelasma
Xanthelasma, or yellow fat deposits under the skin near the inner corners of both upper and lower eyelids, can result in yellow deposits of fat that build up over time and eventually coalesce, becoming unsightly and interfering with proper lid functioning (ptosis). It may be noncancerous lesions; these benign lesions usually go away on their own over time.
Xanthelasma palpebrarum is a form of xanthelasma that typically appears as well-defined, soft velvety lesions near the inner corners of eyelids. Most often female, this form typically affects individuals over 40. Though these lesions do not harm individuals directly, they do signal abnormal blood lipid levels and should prompt consideration of familial hypercholesterolemia as possible cause.
Other types of xanthelasma are equally widespread and can appear anywhere on the body; however, they typically manifest as more diffuse patches of discolored fat with no clearly-defined borders that spread throughout. They can either be flat or raised in texture and are frequently associated with diabetes, liver cirrhosis or familial hypercholesterolemia.
These fatty deposits consist of foamy histiocytes in the superficial dermis and contain nonmembrane-bound lipid vacuoles, cholesterol crystals and lysosomes that do not adhere to membranes. They differ from other cutaneous xanthomas by being located perivascularly without signs of fibrosis.
Though xanthelasma lesions aren’t medically necessary, patients seeking removal for cosmetic purposes may choose treatments such as surgical excision, laser therapy or topical trichloroacetic acid to eliminate them. Alongside such procedures it may be beneficial to implement a regimen designed to lower lipid levels in order to decrease risk of recurrence of lesions.
Although cholesterol has a bad rep, it is an essential nutrient essential to the healthy functioning of our bodies and minds. Though high cholesterol levels pose a major risk factor for heart disease, they can be managed through diet changes, exercise, medication or both in order to decrease the amount of lipids in our bloodstream and prevent degenerative conditions like xanthelasma from appearing around eyes and other parts of body; treating this early could prevent complications later.
Corneal Arcus
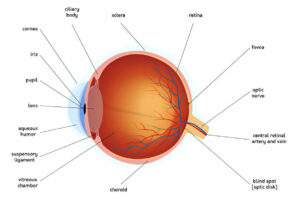
The cornea is the transparent outer surface of your eye that covers your pupil and iris. Usually transparent, its transparency allows your eye color to show through. But over time arcus senilis (ring of fatty deposits in outer edges of cornea) may form. While this condition usually doesn’t indicate high cholesterol levels in bloodstream; if seen among people younger than 45, however, it may indicate familial hyperlipidemia – an inherited condition which increases risk for cardiovascular disease.
Condition is associated with dry eye syndrome, which can lead to discomfort and vision problems, as well as increasing your risk for glaucoma – where fluid from the front chamber builds up and presses against optic nerve causing pain or blindness in one or both eyes.
Secondary Lipid Keratopathy (LK) occurs when an arcus becomes denser, becoming visible as a circular deposit on a corneal blood vessel, often appearing as an opaque spot near it. This condition may result from systemic disorders that impair lipid metabolism such as fish-eye disease or Tangier Syndrome or herpetic corneal infections as well as medications like gold, chlorpromazine, or clofazimine which interfere with metabolism of fats in the eyeball or medications such as these; the latter three may even play a part.
Another symptom of herpetic corneal ulcer is a white haze in the center of cornea. This indicates an infection, and could potentially cause pain as well as scarring, visual disturbances and permanent blindness if left untreated.
Studies indicate that arcus senilis may be linked to central corneal thickness (CCT) and intraocular pressure in people over 50, although these associations aren’t always significant; other factors like age, ocular health and cardiovascular risk should also be taken into consideration before using this sign of high cholesterol levels as a screening tool for coronary heart disease. Other signs that indicate high cholesterol levels include xanthelasmas and cataracts – so if these signs exist for you it would be prudent to consult a medical practitioner for an eye exam as well as blood test in order to monitor your cholesterol level levels accurately.
Retinal Vein Occlusion
Blockages in retinal veins prevent blood from transporting oxygen and nutrients necessary to nourish retinal tissue and nerve tissues in the eye, creating retinal vein occlusions. They may be caused by clots or abnormalities causing narrowing or closing, and may affect any part of the retinal landscape – from its main vein, such as central retinal vein occlusion (CRVO), to one of many smaller branched veins such as branch retinal vein occlusions (BRVOs).
Retinal vein occlusion can result in some mildly discomforting vision blurring or black spot in the center of your eye known as macula, while severe blockages can cause sudden loss of vision along with bleeding in the eye or leakage from capillaries in retina due to pressure build up and fluid leakage from capillaries in retina caused by pressure build up.
Vein occlusion usually results in vision loss that improves over time, though in certain instances vision may remain blurry and distorted even after treatment has begun. This may be because swelling of the macula (cystoid macular edema) worsens and could potentially result in permanent damage to your vision.
As soon as you notice any change in your vision, it is vital that you visit a physician immediately so the condition can be diagnosed and treated if serious. Retinal vein occlusion treatments include injecting medication directly into the eye such as steroids or anti-VEGF drugs in order to reduce swelling while also stopping fluid from seeping into your vitreous humor and worsening your vision.
Risk factors associated with retinal vein occlusions include high blood pressure, cholesterol levels that exceed healthy thresholds, diabetes and other health problems that increase the likelihood of narrowed or hardened arteries or blood clots in blood vessels. It may also be related to inflammation eye diseases that lead to abnormal new blood vessels forming on either retina or iris and could eventually rupture, leading to vision loss.
Diabetes-Related Retinopathy
Diabetes-related eye disease, also known as diabetic retinopathy, occurs when long-term diabetes damages the small blood vessels found at the back of the eye called retinal blood vessels, leading them to leak or bleed and eventually leading to vision loss or blindness. If someone’s glucose levels remain unmanaged for extended periods, diabetic retinopathy becomes increasingly likely.
If you have diabetes, yearly dilated eye exams or as directed by your physician will help detect and treat any diabetic retinopathy present – this will prevent vision loss or blindness associated with diabetes.
High blood sugar levels damage the tiny blood vessels that provide oxygen and nutrients to the retina, leading to leakage or bleeding from these blood vessels, causing swelling of the retina and deposits called hard exudates which interfere with normal vision and increase risk of glaucoma. If these deposits cause macular edema it’s crucial that it’s addressed immediately so you don’t lose your sight!
As diabetic retinopathy progresses, the retina will send signals to the body to produce new blood vessels to restore adequate blood flow to the retina. Unfortunately, these new blood vessels often form abnormally and can bleed, scar or block completely; this serious condition known as proliferative diabetic retinopathy can result in vision loss or blindness.
Diabetes-related retinopathy has been shown to disproportionately impact certain groups. African Americans and Hispanics are especially likely to develop diabetic retinopathy.
Reducing your risk of diabetic retinopathy involves maintaining stable blood sugar levels, quitting smoking and managing cholesterol levels responsibly, as well as regular visits to your eye doctor for a dilated eye exam and retinal photography assessment. Your physician can then tell if treatment for diabetic retinopathy is required as well as laser surgery procedures that could potentially prevent vision loss.