If you experience sudden, painless loss of vision in either eye, it should be evaluated by a retina specialist as soon as possible. With timely treatment, this condition may often be reversed.
A 79-year old male patient presented with sudden loss of right visual field and associated floaters. He was an insulin dependent type 2 diabetic with history of hypertension and hyperlipidemia; fundus examination revealed central retinal vein occlusion (CRAO).
1. Retinal Vein Occlusion (RVO)
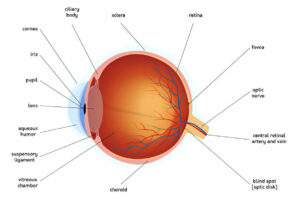
The retina is a light-sensitive layer located at the back of our eye that takes in visual information and transmits it to our brain for interpretation. Blood vessels responsible for transporting oxygen and blood away from retina are vital, but can become blocked due to blood clots. When this happens, vision becomes impaired due to insufficient blood flow to retinal cells that die-off; this condition is known as retinal vein occlusion (RVO).
There are two forms of retinal vein occlusions, Central Retinal Vein Occlusion (CRVO) and Branch Retinal Vein Occlusion (BRVO). CRVO occurs when a blood clot blocks blood flow through a retinal vein, increasing vascular pressure and swelling within the retina causing hemorrhages, vision loss, cystoid macular oedema or cystoid macular oedema to develop. Conversely, BRVO can occur when cholesterol plaque breaks off from hard arteries in the neck before travels directly towards the retina where it clogs one of its veins, although much less severe as only affects peripheral parts of retina.
All forms of retinal vein occlusions can typically be treated using medication, laser and injections. Medication reduces swelling while laser treatment uses high-intensity beams of light to seal leaky blood vessels and shrink abnormal ones; injections with anti-VEGF (anti vascular endothelial growth factor) drugs help promote healing while also helping avoid fluid build up in the eye.
Retinal vein occlusions occur most commonly among people over 60 with other systemic conditions, including hypertension, heart disease, elevated cholesterol and diabetes. Up to 10% of cases can be traced back to giant cell arteritis which reduces blood flow to the retina.
Patients suffering from severe occlusions may require close monitoring over an extended period, however if their symptoms can be managed through medication and injections vision can be saved and patients can expect a good long term visual prognosis.
2. Central Retinal Artery Occlusion (CRAO)
Blocked retinal arteries can result in sudden vision loss. It may affect one eye or both eyes; usually central field vision (field of vision) is affected, sometimes color vision changes occur as well. Although it usually doesn’t cause pain, peripheral fields might experience blurriness from this condition and patients may describe blurriness as well; its absence can help distinguish it from retinal detachments which often causes sensations of discomfort in their eyeball.
Central Retinal Artery Occlusion (CRAO) is an ophthalmic emergency, often described as the equivalent of cerebral stroke. As many as 7 out of every 10 patients will suffer profound and acute visual loss – usually leading to functionally blinding vision (20/400 or worse). This has been linked with subsequent cerebrovascular events, ischaemic heart disease and decreased quality of life; so treatment often includes high dose systemic corticosteroids once diagnosis has been confirmed.
Blockage of the central retinal artery generally impacts all retinal areas; in about 15 percent of cases, however, an obstruction may only impact one branch retinal artery and only supplies part of either half of the retina; this may preserve some vision for patients affected.
Doctors can identify this condition by performing a visual eye exam using an ophthalmoscope and reviewing other health issues affecting blood vessels, such as high blood pressure, diabetes and heart disease, to see if they could be connected. They will likely request routine blood testing to measure hemoglobin thickness which provides an indicator of how well the blood flows; they can also prescribe anticlot medication to stop further vision loss from this condition if necessary. Unfortunately it’s difficult to restore vision lost from this condition; however treating its source could prevent future issues from manifesting itself.
3. Blood Clots
Blood clots are gel-like clumps that form to seal small cuts or breaks in blood vessel walls to stop bleeding and speed healing. Most blood clots dissolve on their own as the body heals; however, in rare instances blood clots form within vessels without dissolving. Clots may form anywhere in the brain, heart, kidneys, lungs and limbs as well as in arteries or veins in these locations – excessive clotting may be caused by diseases, conditions, gene mutations or medications affecting these organs or vessels.
Deep Vein Thrombosis (DVT), in which blood clots form within one or more large veins – typically located in one’s leg or arm – without treatment can result in pulmonary embolism (PE). DVT and PE symptoms include swelling, pain, tenderness or redness at the affected site as well as difficulty breathing and coughing up blue-tinged mucus in this part of their bodies.
Doctors specializing in treating blood clots can help detect these issues early. They will examine a person’s medical history and conduct a physical exam before ordering blood tests to monitor levels of specific proteins that help facilitate clotting processes.
If a doctor suspects you of excessive blood clotting, they will prescribe medicines known as anticoagulants or blood thinners to either prevent or treat it. It is important to take them as directed; otherwise your physician might use catheter-directed thrombolysis or thrombectomy as an additional approach to remove an existing blood clot.
Reducing your risk for blood clots begins by staying mobile during any periods of immobility, such as surgery or bed rest. Try getting up and moving around as often as possible during surgery or bed rest; for car trips try stopping to walk around as often as possible; when traveling by car consider stopping every few miles for walks around or stops and walks during long trips; avoid long term use of sedatives; drink plenty of fluids regularly and remember if there is a family history of blood clots you are at an increased risk.
4. Ocular Stroke
Ocular stroke occurs when blood flow to the retina (the back of the eye) is interrupted due to a blockage. Much like brain stroke, an ocular stroke usually involves blood clots but other problems like inflammation or trauma could also contribute. A sudden painless vision loss (usually the left eye) or reduced vision area could indicate this is happening and must be treated quickly as this constitutes the equivalent of cerebral stroke.
At the core of any patient evaluation is an in-depth history and physical exam, inquiring as to whether their symptoms are bilateral or unilateral – the former might indicate an eye pathology while bilateral involvement might suggest neurologic causes. Furthermore, it’s essential that any symptoms being experienced are transient or persistent and how long they have been occurring for.
Ocular strokes typically result from a blood clot forming in either an artery or vein. The type of clot determines its impact, and any subsequent vision loss.
At times, blood clots in the central retinal vein (the main blood vessel in the eye) may result in sudden, painless and permanent loss of vision – known as central retinal artery occlusion or CRAO and considered an eye medical emergency that must be immediately treated at a comprehensive stroke center.
Preventing this condition involves taking steps to manage blood pressure, cholesterol levels and other cardiovascular disease risk factors. Middle aged and elderly adults in particular should strive to lead a healthy lifestyle in order to lessen the chance of eye stroke resulting from vascular conditions.
Notably, symptoms of CRAO could be the result of having patent foramen ovale, an underlying heart condition which increases your risk for future recurrent eye strokes and should be checked out by your cardiologist.